Therese Taylor was fifty-two when she had her first clinical breast exam, in the office of a new family doctor. He recommended that she go for a mammogram. After she shrugged the suggestion off, protesting that she wasn’t interested, he told her he’d found a lump in her right breast. Suddenly, she was confronting the thing that every woman dreads. So she complied. She went for the mammogram a few days later, in the first week of October 2011. No lump in the right breast was visible on the X-ray. Little white specks showed up in several places in the image of the left breast, however—flecks of calcium that indicate the presence of malignant cells. These “microcalcifications” meant that she needed to see a surgeon. Ten slow, anxious days after a biopsy, the surgeon had her back in his office and gave her the diagnosis. She had DCIS.
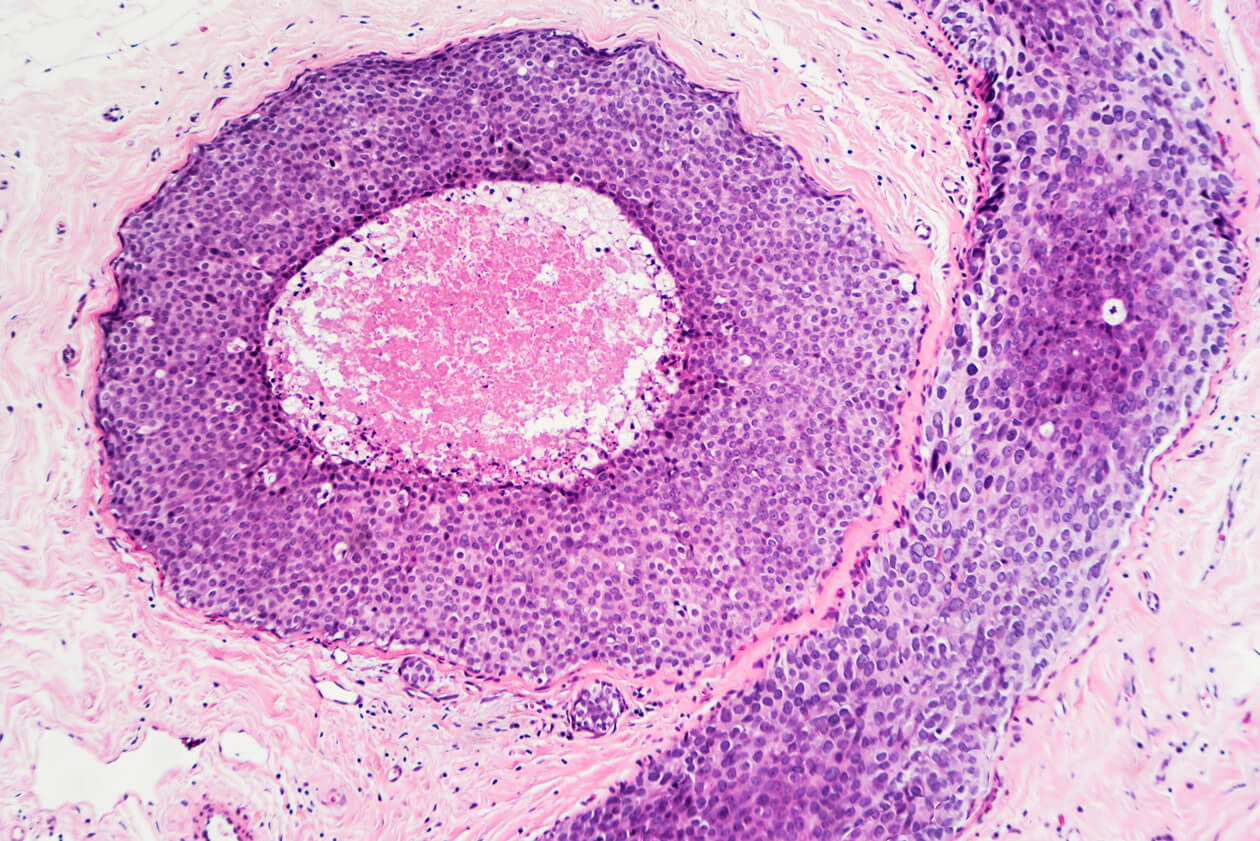
DCIS—or ductal carcinoma breast cancer—is diagnosed when malignant cells are confined within the milk ducts of the breast. When a tumour breaks through the walls of the ducts and invades surrounding tissue, it becomes invasive breast cancer. On a mammogram, DCIS can look like a string of calcium specks, sometimes lined up, sometimes following a squiggly path, and sometimes spread more diffusely, in a feather-like pattern. It can occur in different parts of the same breast. The calcium results from cancer cells dying off. Sometimes DCIS is a solid tumour within the milk duct, but it’s rarely large enough to feel, and because of this, almost all DCIS is diagnosed as a result of a mammogram.
The condition was first described a century ago by the surgeon and pathologist Joseph Colt Bloodgood at Johns Hopkins University, but it was only when mammography screening started to become popular in the 1980s that DCIS was routinely detected. Because of mammography, the incidence of DCIS in the United States increased more than sevenfold from the mid-1970s to the end of the 1990s. Today, it’s estimated that between 20 and 30 percent of cancers detected in screening mammograms are DCIS. In the United States, over 50,000 new cases of DCIS are diagnosed every year, most in women between the ages of fifty and sixty.
Yet it’s not clear what DCIS really is. Historically, DCIS has been considered a precancerous condition, a precursor of invasive cancer, in the way that some suspicious cells in the cervix discovered in a Pap test are considered precancerous. Therefore, to prevent DCIS from becoming invasive, the standard protocol is to excise it. This practice is becoming increasingly controversial because most DCIS will not progress to invasive cancer, but the difficulty is knowing which ones will and when.
So multitudes of women are undergoing lumpectomies and, depending on how widespread the DCIS is in the breast, full mastectomies for a poorly understood and unpredictable precancerous condition that might not cause any harm. Is it even fair to call it precancer? Some experts argue that it isn’t and that calling it a carcinoma is mislabelling if not misleading. Thanks to mammography screening, the ability to detect DCIS is contributing to overdiagnosis.
Therese Taylor didn’t know any of debate about DCIS when her surgeon told her she needed to have her breast removed. DCIS was “consistent with cancer,” he said. She didn’t ask him to explain what he meant, thinking it was just a nice way of saying “you’ve got cancer.” She went home dazed by the news. Taylor returned for a second consultation a few days later, this time with her husband, and asked what stage her cancer was. “Stage zero,” the surgeon said. Taylor didn’t think to ask what that meant either. The surgeon said he was pretty sure she wouldn’t need radiation or chemotherapy, but she had to have a mastectomy because the DCIS appeared to be in too wide an area to capture with a simple lumpectomy. “It was numbing,” Taylor says. “The worst part was telling the kids and wondering how worried about it they were going to be.”
Taylor had been living a comfortable life in a spacious suburban house in Mississauga, Ontario. When she was diagnosed, her eldest son was in college, the younger one was in high school, and her daughter was twelve. The family had moved to Mississauga in 2002, when the house was relatively new, built less than fifteen years before. Soft spoken, small in stature, and dressed conservatively in brown, Taylor gives the impression of someone entirely unassuming. She’s not a person you’d notice in a crowd. Her long brown hair hangs below her shoulders, with a fringe that frames a small face that is warm but has an earnestness that suggests a person with convictions.
Taylor received her diagnosis on October 28. She had the mastectomy two weeks later, on November 14. Three weeks after the operation, she saw the surgeon once more so that he could check on her wound. That was the first time she heard the word precancer.
A few years after the mastectomy, Taylor heard something on the radio about overdiagnosis of breast cancer and, later that night, saw a television news story. She needed to know more and launched into research. One of the first things she came across was a 2009 Associated Press story in the Toronto Star headlined “Milk Duct Tumours Not Really Cancer.” The story was about a comprehensive report from the National Institutes of Health (NIH) attempting to sort out the controversy, confusion, and uncertainty around DCIS.
In September 2009, leading breast-cancer researchers had gathered at the Natcher Conference Center on the NIH campus to review and discuss the current science around detecting and treating DCIS. At the end of the four-day meeting, they issued what they titled the “State-of- the-Science Conference Statement on Diagnosis and Management of Ductal Carcinoma in Situ.” A DCIS patient would not get much comfort from the twenty-page document noting that “the natural history of DCIS is poorly understood” and management and diagnosis of it are highly complex. Many unanswered questions remained, the researchers said. Most vexing was (and still is): How can we know when DCIS will develop into invasive breast cancer?
Pathologists had determined that there are different “grades” of DCIS depending on the patterns created by the proliferation of cancer-like cells and how densely packed they are within the duct. The most worrisome is high grade, when the cells become compacted enough to plug the duct and the cells in the centre become starved of nourishment and die, resulting in what’s called comedo necrosis. The evidence was that high-grade DCIS was “strongly associated” with the risk of developing invasive breast cancer. But an association is not cause and effect. Rather, it’s an observation that two things are happening at the same time and are possibly connected. Nor was the science strong enough to say only women with high-grade DCIS should be treated.
And what should the treatment be? Breast-conserving surgery (lumpectomy)? Full mastectomy? Lumpectomy combined with radiation? Drugs such as tamoxifen, sometimes used to prevent invasive cancer? The questions the scientists were trying to answer in 2009 still have no definitive answers. The standard of care for DCIS today, as then, calls for surgery. If it’s contained in a small area, a simple lumpectomy might suffice, and sometimes that’s done along with a procedure to check for any immediate involvement of lymph nodes. But if it is spread out to the point that a lumpectomy would remove so much tissue that it would be cosmetically unacceptable, a complete mastectomy is standard. Mastectomies are done in about a quarter of DCIS cases.
Therese Taylor’s DCIS was classified as high grade and was detected in more than one place in her breast. Her surgeon was following the protocol of the time and probably what he understood to be best for his patient. She doesn’t understand, however, why there was such a hurry. She feels she was coerced, first by the family physician who persuaded her to go for a mammogram, even though she herself couldn’t feel the lump he said he’d found, and again by the surgeon who rushed her to the operating room, leading her to believe invasive disease threatened her life.
Taylor feels that if she had known there was a controversy and understood more about the condition, she might have made a different choice. She certainly would have thought about it longer. Taylor opted not to undergo another surgery for breast reconstruction, so she lives with a scar across her left breast that is a constant reminder of a loss she feels deeply, not with anger but with sadness. For a long time, she wore her hair long enough so that she could brush it down over her disfigurement. “Don’t look down,” she would tell herself as she stood in the shower. “Don’t look down.”
The NIH report on DCIS was, for many, an eye opener. The NIH state-of-the-science panel consisted of fourteen members representing oncology, radiology, surgery, obstetrics and gynecology, epidemiology, biostatistics, pathology, nursing, preventive medicine, and social work. In addition, twenty-two experts were invited to speak to the panel. Karla Kerlikowske was one of the first, there to discuss the prevalence of DCIS.
Kerlikowske is a physician in internal medicine and professor of medicine specializing in epidemiology and biostatistics at the University of California, San Francisco. She has published widely on breast imaging, the epidemiology of invasive breast cancer, DCIS, and predicting the risk of invasive breast cancer. Kerlikowske told the panel screening mammography had led to a DCIS “epidemic.” Somewhere between 17 and 34 percent of all breast-cancer cases found through mammography were DCIS. Yet despite twenty years of detecting DCIS on mammograms, the incidence of invasive breast cancer had not declined. If early detection of DCIS worked, it should have resulted in consistently fewer cases of invasive cancer, and that wasn’t happening.
Kerlikowske is articulate and plain spoken, and she addresses a crowd in the way that you imagine she might speak to a patient, clearly and confidently. In a lecture for the University of California’s mini medical school, shortly before the NIH panel on DCIS, she provided a detailed but accessible breakdown of what scientists knew. The essential facts haven’t changed. Only 15 percent of DCIS cases progress to invasive cancer within ten years. Even more encouraging, only 2 percent of women treated for DCIS will die within ten years. Kerlikowske suggests that means one of two things: either the surgery and treatments for DCIS are effective or indolent malignancies that would never cause harm are being treated unnecessarily. In the absence of clinical trials comparing women treated for DCIS to a control group of untreated women, it isn’t possible to determine which of the two it is.
Kerlikowske prefers to think of DCIS as a marker of breast-cancer risk, not a true precursor. Treating DCIS is not the same as removing polyps during a colonoscopy, which does reduce the incidence of colon cancer, she explains. A colonoscopy can be seen as a preventive measure. Mammography is not. It’s not about decreasing the incidence of disease; it’s only about finding it.
The NIH panel ended its meeting with a catalogue of research questions aimed at accurate identification of risk for invasive cancer and a better understanding of the biology of DCIS. It also dealt with the psychological impact of diagnosing DCIS as if it were a true cancer. Women who have it “should have access to the best available information and guidance to help make decisions about their care,” it urged. The panel’s final statement recognized the unwarranted anxiety surrounding a condition with such a low mortality rate. “It is also important,” the statement read, “for the medical community to consider eliminating the term ‘carcinoma’ in this disease, as DCIS is by definition not invasive—a classic hallmark of cancer.”
In an effort to find solutions to the problem, the US’s National Cancer Institute, called a meeting of experts to assess this overdiagnosis in 2012. After a two-day brainstorming session, the participants decided that their first recommendation was to change cancer terminology. They adopted a new name for noninvasive cancers and precursors: indolent lesion of epithelial origin, or IDLE.
Epithelial refers to the cells that line the cavities of the body: the stomach, most organs, intestines, esophagus, ducts, and glands. The skin is also made of epithelial cells. The NCI experts agreed that if the medical community learned to see indolent cancers as IDLEs, they’d see them differently and approach them less aggressively. Patients would also be less afraid. A common dictionary defines idle as “not active or in use.” IDLE might be a fitting acronym to describe something that is not yet cancer or is cancer that is not progressing. But, so far, DCIS remains ductal carcinoma in situ.
DCIS continues to present a clinical dilemma. Ten-year survival after treatment for DCIS remains in the 98 percent range. It’s estimated that one in every thousand mammograms finds DCIS, making up a quarter of all breast cancers caught by screening. In the United States, it’s been calculated that by 2020, 1 million women will have had a DCIS diagnosis. Although the annual incidence levelled off in the early 2000s, probably due to the rate of mammography screening reaching its maximum point, there are up to 60,000 new cases each year. The natural history of the condition is still unknown. It’s not understood how and when DCIS progresses to invasive cancer. And if it’s a precursor to invasive cancer, why don’t its detection and surgical removal have a correlating impact on the incidence of invasive cancer? In the absence of answers, lumpectomies with or without radiation or mastectomies remain the medically recommended course. But perhaps not for long: both doctors and patients are advocating for change.
Desiree Basila is a high-school science teacher in San Francisco. She was also doing ballet, and dance was taking up a lot of hours. She hadn’t had a mammogram in about seven years. When she was fifty-two, an injury kept her away from physical activity, and with time freed up, she thought, Why not go for a mammogram? It was June 2007. The mammogram showed an abnormality, which meant that she had to see a surgeon, but she didn’t think much of it, as others in her family had had cysts. She’ll never forget the emotional shock and the incredible animal fear when she got the news. The surgeon walked briskly into the room, snapped the X-ray into the viewer, and said, coldly, ‘Yes, it’s cancer.’ It was DCIS. Without giving Basila time to process that information, the surgeon said she was going on holiday in two weeks but had a slot open for a mastectomy. She wanted to perform a biopsy first thing the next morning.
Basila, in a panic about having cancer, went for the biopsy. In an examination room, she happened to pick up a booklet about DCIS that had perhaps been forgotten by another patient. She began to read it, took it home, and scoured the internet for more information. After a little research, she said to herself, “Wait a minute. You want me to go in and have my chest chopped off, as a prophylactic measure against getting invasive cancer, and to your knowledge that only happens 20 to 40 percent of the time? That’s not going to happen.”
With the help of her primary-care physician, she wriggled through the rules of her health-maintenance organization to secure a consultation with another doctor, three months later, in September. That doctor was Shelley Hwang, chief of breast-surgery oncology at the University of California, San Francisco, and a leading DCIS researcher.
Basila was seeing the best, and she was hopeful. She had a long list of questions and a lot of ideas about approaches they could take to avoid surgery. Coupled with the extensive research she had done, her background in science made her curious and willing to try different options. But, at first, the meeting did not go well. Basila found Hwang cool and aristocratic. For her part, Hwang was looking at a woman with a five-centimetre lesion in her breast. Because the mass was large, a lumpectomy would not be good cosmetically, and like the first surgeon, Hwang recommended a mastectomy. Basila persisted with her questions. Hwang kept saying she needed a mastectomy. Disappointed, frustrated, Basila decided that the conversation was going nowhere and got up to leave. She plucked her coat from the hook on the door, but just as she was walking out, she turned and asked, “What if I just don’t do anything?”
She threw it out there, expecting Hwang to say, “Well, you could do that, but I wouldn’t advise it.” Then she’d write on Basila’s patient record that she’d refused treatment. Instead, Hwang nodded and told her some people were choosing to do that. Basila walked back in and sat down, and suddenly the whole conversation changed. Hwang, she says, just lit up and started talking about her research. She was doing what’s called a proof-of-concept trial, where DCIS patients took the drug tamoxifen for three months before undergoing surgery. Basila became part of that trial, but at the end of three months, she still didn’t want surgery and dropped out.
She continued taking tamoxifen, however, and for a while, Hwang saw her every week.
After eight months, Basila gave up on tamoxifen because she felt moody and exhausted. Finally, Hwang agreed to active surveillance: every six months, Basila would have an MRI and a mammogram. (The term active surveillance is considered a better way to describe a watch-and-wait routine, which patients could infer means doing nothing.) Basila underwent extensive monitoring. Ten years later, the DCIS remains stable, and she goes for a mammogram just once a year.
As uncomfortable as she was with leaving Desiree Basila’s particular DCIS untreated, Shelley Hwang was also uncomfortable with growing evidence that many DCIS cases were aggressively overtreated. Like other breast surgeons, she noticed that more women were choosing to have a double mastectomy even though the preinvasive cells existed in only one breast. Patients believed cutting off the unaffected breast increased the chances of cancer never recurring, or they chose it for cosmetic reasons. When she met Basila in 2007, she and her colleagues worried about the potential for needless physical and psychological damage to women who would never have come to them were it not for mammography screening. Not that they thought screening was bad, but finding DCIS was an unintended consequence that was now a big problem.
Eventually, Hwang would entertain the possibility of active surveillance as a standard protocol. What she had noticed about double-mastectomy rates turned out to be real. In the 1990s, a double mastectomy for DCIS was rare. By 2010, 8 percent of women with the diagnosis chose that course, despite the lack of evidence that this drastic measure made any difference to their survival. In 2011, Hwang moved to North Carolina to become chief of breast surgery at Duke University, where she continued her DCIS research. After some preliminary data showed no difference when women with the most favourable kind of DCIS chose active surveillance, Hwang secured funding for a clinical trial.
The trial, known as COMET (comparison of operative to monitoring and endocrine therapy), began recruiting in 2017 and will continue until 2021. Nine hundred women with low-risk DCIS will be randomized to either the standard protocol or to active surveillance and will be followed for two years. In addition to monitoring these women closely to see how many go on to have invasive cancer, the study will collect blood and tissue specimens and do genomic sequencing in the hope of learning how to identify which patients are of such low risk that they can safely opt out of surgery. Says Hwang, “This is a very important issue, and it’s not okay to continue treating patients with very aggressive treatments because we don’t know what the alternatives are.”
Hwang’s pioneering work earned her a place among Time magazine’s top 100 most influential people in the world for 2016. Time co-listed her with Laura Esserman, also a surgeon and breast-cancer oncology specialist and, since 1996, director of the Carol Franc Buck Breast Care Center at the University of California, San Francisco. Esserman has been called a rebel because she’s long argued that cancer screening has created a situation where low-risk breast and prostate cancers are overdiagnosed and overtreated. Especially concerned about DCIS, she was an early advocate for active surveillance and, as early as 2009, recommended that DCIS be categorized not as cancer but as an IDLE, to classify it as low risk and possibly not needing treatment. “Much of what we call cancer is not destined for an inexorable progression to metastasis and death,” she wrote in 2010. “We can no longer say that we must intervene because we cannot tell the difference.”
Some of Esserman’s research has focused on how to improve screening by determining who should be screened, at what age, and how often, depending on individual risk. Women don’t want more screening, she says, but they do want better screening. One mammogram in ten produces a false positive result. The psychological distress that results is one problem; false positives also make women want to give up on screening. The United States is the only country where it’s standard to attend screening beginning at age forty, yet the breast cancer mortality rate is not better than in countries with less screening, Esserman notes. And overdiagnosis is a growing concern. She argues that current screening practices rest on the decades-old assumption that all women have the same risk for the same kind of breast cancer. Insisting that women deserve better than a one-size-fits-all approach, she’s launched a massive new study called the WISDOM trial (women informed to screen depending on measures of risk). Her plan is to re-examine screening in light of what we know today: that different breast cancers vary in terms of size, time of onset, rate of growth, and probability of metastasis. Treatments are becoming personalized, so why not personalize screening?
Regular screening means annual mammograms beginning at age forty. Tailored screening means that the age at which a woman would begin screening, and how often, would depend on risk factors determined by an extensive questionnaire regarding family and health history and a saliva test to look for genetic factors. A primary goal of the study is to determine whether risk-based screening is as effective for cancer detection as annual screening.
Esserman hopes that the findings from the study will quell the current screening debate. But risk-based screening is in itself contentious. Breast-screening advocates worry that if it leads to fewer people being screened, cancers will be missed because, they argue, in the majority of cases, identifiable risk factors, such as dense breasts or a history in the family, are not present, especially in younger women.
Esserman’s approach to risk-based screening, however, also has critics among screening skeptics. Their concern is that genetic risk scores might scare women without having much impact on mortality, possibly leading to more screening instead of less.
In the latter camp, count Steven Narod. He is not a fan of mass population screening and has written papers on overdiagnosis. But what he’s working on these days raises some other questions about DCIS and its role as a precursor, or not, of invasive cancer. Narod is an epidemiologist, head of the Familial Breast Cancer Research Unit at Women’s College Hospital and a professor at the University of Toronto; the hospital’s website boasts that he is the most-cited researcher in the field of breast cancer, with more than 800 peer-reviewed publications.
In JAMA Oncology in August 2015, Narod published what one headline dubbed a “blockbuster” study. It was about breast-cancer mortality after a diagnosis of DCIS. He and his research team analyzed twenty-year data from a national US cancer database called Surveillance, Epidemiology, and End Results, better known as SEER.
They looked at close to 110,000 women diagnosed with DCIS from 1988 to 2011 to see how many later died of invasive breast cancer. Three main findings emerged. First, the mortality rate after twenty years was low: only 3.3 percent of women diagnosed with DCIS died of invasive breast cancer. Good news, so far. They also found that regardless of how the women were treated—lumpectomy with radiation, lumpectomy without radiation, or mastectomy—the mortality outcome after twenty years was the same. A few months later, Shelley Hwang’s research team would support this important finding in another paper.
The third finding was the “blockbuster” and the one Narod thinks is the most clinically significant. More than half, 54 percent, of the women who died of breast cancer after twenty years did not experience invasive cancer in either breast. In other words, even though the DCIS had not penetrated past the milk ducts and did not result in invasive cancer in the breast, invasive breast cancer showed up elsewhere in the body. Could this mean that the cancer had spread even before theDCIS was removed? It was a stunning observation and, for Narod, mind blowing, raising even more questions than ever about what DCIS really is.
The point of finding DCIS through screening, and treating it, has been to stop a precursor of invasive cancer from plundering healthy tissue. But as Narod wrote in his paper, “If DCIS were truly a non-invasive precursor of breast cancer, then a woman with DCIS should not die of breast cancer without first experiencing an invasive breast cancer” in a breast. “It is often stated that DCIS is a pre-invasive neo-plastic lesion that is not lethal in itself,” he noted. “The results of the present study suggest this interpretation should be revisited.” He suggested that DCIS should be considered to behave no differently than small invasive cancers. Most small invasive cancers don’t turn out to be lethally aggressive, but some do. Removing those doesn’t mean you’ve prevented breast-cancer death, he says. But proposing that metastasis might have occurred directly on a path from DCIS to some other part of the body, skipping past the steps to invasive cancer in the breast and involvement in the lymph nodes, is a radical idea.
Hwang points out that the SEER data Narod looked at have limitations because they don’t provide specific information about patients. It’s possible that invasive cancer within the breast might have been missed. The theory would need to be tested biologically. It comes back to the need to really understand the natural history of breast cancer.
Narod suggests that perhaps all this time we’ve been chasing the wrong squirrel. “What we think of as cancer is not cancer,” he suggests. “What we’re seeing in the breast is only a shadow on the wall and doesn’t really predict whether the women will die.”
The DCIS research stimulated a curiosity that resulted in a set of theoretical and provocative arguments Narod and his colleague Victoria Sopik developed in Breast Cancer Research and Treatment early in 2018. Throwing conventional wisdom aside, they proposed that cancer cells in the breast are not the source of distant metastases and that “if a breast cancer is going to metastasize it will have done so before it is clinically apparent.” They proposed that breast cancer does not develop in an orderly, sequential fashion but results from a more dynamic process. Although the hypothesis will seem “out there” to many, it builds on some of the things scientists have wrestled with for decades—for example, how to explain why there is no difference in survival rate whether the surgery choice for DCIS is lumpectomy or mastectomy.
If Narod is right, what could that mean for breast screening? He explains that, yes, the earlier a cancer is identified, the better the survival. But that could be for two reasons. “As cancers get big, they acquire the potential to spread. Or, as cancers get aggressive and spread, they grow faster.” The first supports screening; the other doesn’t. “We think big cancers are more likely to kill you than small cancers, because cancers that are likely to kill you get big quickly. No one disputes the fact that the larger cancer is the one that kills you. The question is, Can I prevent that death by finding a particular cancer when it’s smaller?” Bad cancers tend to get big, he says, but that doesn’t necessarily imply logically that finding the cancer when it was small can prevent the death.
Narod’s opinion is that early detection doesn’t work. If screening worked, if stopping DCIS from progressing worked, the number of new invasive breast cancers should go down. But it hasn’t—it has led to overdiagnosis and overtreatment.
Adapted from Conspiracy of Hope: The Truth About Breast Cancer Screening. Copyright © 2018 by Renée Pellerin. Reprinted by permission of Goose Lane Editions.